Throughout history, many different names have been associated with CRPS. Some of these include reflex sympathetic dystrophy, causalgia, peripheral trophoneurosis, minor traumatic dystrophy, atrophie de Sudeck, and algodystrophy, to name a few. For the purpose of simplicity, we will refer to RSD/CRPS as simply CRPS henceforth. Many more women seem to suffer from CRPS than men (about 75 percent more). CRPS has been diagnosed in very young children (so much for it being a “manufactured” condition) and usually peaks around midlife. It is a chronic disease that often worsens over time. Alarmingly, 35 percent of sufferers eventually report symptoms throughout the body. The disease may remain localized, spread slowly over years, or progress rapidly like a wildfire out of control.
Who Can Get CRPS?
While stress (physical, emotional or chemical) causes all disease, it is our belief that CRPS is not the result of one single event or stress, but more like a complicated puzzle, made up of different parts. Stress only affects you adversely physically if you cannot adapt to it. People who suffer from CRPS became overwhelmed to the point that their bodies could not adjust or respond to stress, and CRPS was the unlucky result. Our patients, for whatever reason, (most of the time it is chronic viral infections or childhood trauma) had an imbalanced nervous system prior to developing CRPS. The triggering event is not the cause of the CRPS – it’s just the “straw that broke the camel’s back” allowing symptoms to appear.
How is CRPS Diagnosed?
Although there is no one single definitive test for CRPS, there are a few things doctors look for when diagnosing this condition, and tests that help them to do so. If a patient is lucky, they will cross paths with a doctor well-trained in the diagnosis and treatment of CRPS (most often a neurologist or anesthesiologist).
Diagnosis of CRPS is based on a physical exam and your medical history. Again, there’s no single test that can definitively diagnose CRPS, but the following procedures may provide important clues:
The Three-Phase Bone Scan
X-Rays
Thermogram
Neurologic Tests
Physical Exam
Check out How is CRPS Diagnosed? for a deeper dive into each of these and diagnosing CRPS.
The Old Way: Common Current Treatment Methods of CRPS
Although I am known to be a big proponent of treating the cause rather than the symptom, and I try to teach my patients a mindset that allows them to investigate and examine the root cause of their symptoms, CRPS has been humbling for me as a doctor.
What I mean by this is that even the bravest patient cannot typically survive the sky high pain levels that characterize CRPS without some kind of intervention or help from the outside. CRPS taught me that sometimes, pain relief is not a luxury or a choice, but a necessity for simple survival. That being said, I have been humbled by the bravery I have encountered in many CRPS patients, who will refuse to reach for pain medication unless they are backed against a monstrous wall of pain. Because most CRPS patients have access to vast amounts of pain medications, this truly takes self control.
In this section I will -cover some of the treatments available to CRPS patients today. My list by no means can boast to be all inclusive, but I will try my best to give you a good understanding of your options.
Pros & Cons of the Treatments Available to CRPS Patients Today –
Please note that my opinion of any treatment is often based upon my own research only. It is not my intent to encourage nor discourage you from seeking a specific treatment. My only intent is to supply information in a fair and balanced manner. As with any treatment, you are responsible for researching any possible treatment that you may consider, including its pros and cons.
The use of pain medication in the treatment of CRPS is widely used but somewhat controversial. In the USA especially, pain medications are usually used as the first line of defense when it comes to the treatment of CRPS. However, the successful treatment of CRPS is so elusive and looks very different in each patient, as no one seems to respond the same way. Very often, CRPS patients will tell me that they respond “differently than anyone else” when it comes to pain medications. I suspect that at least part of the reason for this is the MTHFR gene mutation that most CRPS patients seem to suffer from. Remember, this gene mutation will often cause your body to detoxify harmful substances, like medications, at a much slower than normal rate.
Opioids include medications such as morphine, hydromorphone, methadone, hydrocodone and oxycodone and the fentanyl patch, to name a few. Considerable controversy exists regarding the use of opioids for treatment of chronic pain of non-cancer origin, and this is especially true for CRPS. The most popular opinion is that opioids are not very effective in the treatment of chronic pain conditions of a neurologic nature. Currently, there are no well-controlled long term studies showing long term improvement in CRPS patients using opioids. However, many patients suffering from CRPS rely on opioids just to get through the day, and report that it does give them at least some pain relief. In my experience, when successful, opioids will typically lower the CRPS patients’ pain about two points or so on the pain scale.
Side effects caused by the use of opioids are very common and may be dangerous. Common opioid side effects, particularly with higher doses, include constipation, dependency (not to be confused with addiction), nausea, vomiting, cognitive impairment, sleepiness, and trouble breathing. The longer opioids are used, the higher the chances of experiencing side effects and addiction. In some cases, long term use may even lead to something called hyperalgesia, meaning increased sensitivity to pain. Opioid use is very hard on your body, also. Both the liver and kidneys have to work overtime to rid your body of this class of drugs daily. Long term use contributes to cellular toxicity, decreased immune function, and disruption of your hormones.
Lyrica was first approved for the use of fibromyalgia in 2007. Its side effects include weight gain, dizziness, drowsiness, dry mouth, speech disturbances, sinus infections, swelling of feet and hands, infections, headaches, double vision, accidental injury and difficulty with concentration. In more serious cases, patients have reported severe allergic reactions to Lyrica, including hives, blisters, increased heart rate, itching, difficulty breathing and swelling of the face and tongue. Lyrica may interact adversely to other medications, such as sleeping medications or some opioids, such as morphine. It is postulated that Lyrica actually addresses the symptoms of spinal cord pain rather than the indirect symptoms of CRPS. The EU (European Union) approved Lyrica for central spinal cord pain.
While Lyrica is certainly no magic bullet, most CRPS patients report that it relieves their pain at least moderately, although its success varies from patient to patient. Lyrica should never be stopped cold turkey. When my patients complete their treatment or enter the second phase of the intense part of their treatment, and report significant lower pain levels, I always refer them to a physician that can advise them about slowly tapering down their use of Lyrica.
Cymbalta is an antidepressant sometimes prescribed to treat nerve pain and other conditions off label. Similar to Lyrica, it is postulated that Cymbalta (Duloxetine) actually addresses the symptoms of spinal cord pain rather than the indirect symptoms of CRPS. Side effects of Cymbalta include, but are not limited to: blindness, abdominal pain, blistering of skin, blurred vision, loss of consciousness, cold sweat, mental confusion, dark urine, decreased urine output, convulsions, impaired vision, difficulty swallowing, lightheadedness when suddenly standing up, fainting, hives, loss of bladder control, uncontrollable jerking of extremities, shivering, sign of liver damage such as yellowing of the skin and sudden uncharacteristic feelings of excitement you cannot control. Cymbalta should also be tapered down with the help of a physician. Most CRPS patients report a moderate level of pain relief using this medication. Cymbalta may interact with more than a thousand other drugs in a negative way (for example morphine), so make sure that your doctor checks the safety of all your drugs when taken together, not just individually.
There are many other drugs that are prescribed to CRPS patients.
This list includes (but isn’t limited to)
Topamax (an anti- seizure medication),
Neurotin (or Gabapentin, originally developed to treat epilepsy),
NSAIDS,
low dose Naltrexone and many others.
Please understand that of all the groups of chronic pain patients who have the right to reach out for pain medications, CRPS certainly should appear at the top of that list. I do urge you, however, to take every drug you decide to take under very careful consideration. You must never blindly trust any doctor (including myself) or pharmaceutical company, ever. It is your job to be your own advocate.
This means that you must research every single drug you take carefully. Be aware of its potential side effects, negative interactions with other drugs as well as alcohol, and how to quit taking it, should that time arrive. You must also work hard to support your liver with detoxification (not to be done without help), a good diet, and supplementation. Last but not least, never take a medication “just because”. What do I mean by this? Astoundingly often, patients will tell me that they are taking something, even though they really can’t tell if it is helping. If some time has gone by and you cannot tell a difference, why subject your body to this added chemical burden? Only take a medication if you can tell that there is a clear effective benefit while you are taking it.
Calmare therapy disrupts the pain signal by ‘scrambling’ it. It is suitable for severe, chronic, neuropathic and oncologic (cancer) pain patients exclusively using the MC-5A, a computerized medical device. This medical device has FDA clearance. The treatment incorporating this technology, called Scrambler Therapy(ST), uses disposable surface electrodes on the skin (similar but not the same as a TENS unit) to transmit synthetic non-pain information through surface nerve receptors. This treatment applies a low amperage electric signal that is composed of codes recognized and normally used by the brain. These codes enter the body through dermatomes, (or specific areas of the skin known to be supplied by a single spinal root) to the dorsal (posterior) part of the spinal cord and central nervous system (CNS). The new code ‘tricks’ the brain to read a discernable non-pain code as real and generated from itself. When this happens, there is a ‘zeroing out’ of the pain. Through plasticity (the ability of the brain to adapt to change) the brain will then learn to expect, look for and prefer the non-pain code.
This treatment is non- invasive, and should show results fairly soon, if it is going to work. It is typically paid for out of pocket as it is typically not covered by insurance companies. Please note that this is often the case for successful more non- traditional treatments. You can find success stories all over the Internet about this therapy, and also CRPS patients for whom it did not work, unfortunately. Success is often determined by the severity of the case. It seems that patients with one limb responds better than patients in which the CRPS has spread. The one clear drawback appears to be that the treatment will often not last, and patients have to go back for additional treatments, which may be costly over time. Some patients report longer periods of relief and others only short periods.
If this treatment works exactly the way it claims to work, it will merely change the way the brain responds to pain, not the disruption in the CNS. If you do not address the nervous system dysfunction that gave rise to CRPS to begin with, you are still walking around with a ticking time bomb inside your body, that may give rise to other conditions and/or symptoms.
Ketamine, discovered in 1962, is a medication mainly used for starting and maintaining anesthesia. Ketamine may be administered to CRPS patients in one of three methods; It may be used in a low-dose "Awake" version, the "Coma technique", or as an out-patient procedure. The “awake” version is the most widely used procedure today. The patient typically receives a dose of between 20 mg and 35 mg of Ketamine, depending on several factors. The cost of this procedure varies between $10,000 and $50,000 and may be covered by insurance. It was pioneered by Doctor Correll, of Australia, and Doctor Ronald Harbut, of Hot Springs, Arkansas.
The “coma technique” is not FDA-approved for use in the USA. The treatment used to be available in both Germany and Mexico, but the German program was shut down, reportedly after at least one patient passed away after undergoing this procedure. During this procedure, the patient is placed in a deep five day coma, during which they have to be placed on a ventilator. The procedure has almost the same effect on the CNS as hitting “control”, “ALT” and “Delete” on your computer keyboard. It reboots the CNS, often resulting in the pain to massively decrease or disappear, sometimes for long periods of time. The cost of this procedure is in excess of $60 000. The outpatient procedure is not reported to be very effective at all.
One article sums up the way Ketamine works in the following way: "Although Ketamine may have more than one mechanism of action, the basis for using it to treat CRPS/RSDS may reside in its strong ability to block NMDA receptors. Experimental evidence suggests that a sufficiently intense or prolonged painful stimulus causes an extraordinary release of glutamate from peripheral nociceptive afferents onto dorsal horn neurons within the spinal cord. The glutamate released, in turn, stimulates NMDA receptors on second-order neurons that produce the phenomena of windup and central sensitization. It is reasonable to consider that, by blocking NMDA receptors, one might also be able to block cellular mechanisms supporting windup and central sensitization. Ketamine is the only potent NMDA-blocking drug currently available for clinical use. Our interpretation is that an appropriately prolonged infusion of Ketamine appears to maintain a level of Ketamine in the central nervous system long enough to reverse the effects of the sensitization process and associated pain." 42
NMDA (N- methyl-D-aspartate receptor) is a glutamate receptor and ion channel protein found in nerve cells. Glutamate is a nerve cell messenger that causes excitation (excitement) in nerve cells. It may cause harm when its messages become overwhelming. You may say that NMDA is the lock, and Glutamate is the key. When the key unlocks the lock it causes excitement in nerve cells. It this process becomes on going, it may cause chronic pain.
Ketamine is known as one of the most effective treatments for CRPS today. However, all that means is that it is more effective than most other treatments for longer periods of time. Although ketamine has been known to cause remission in some lucky patients, most patients seem to have to go back repeatedly for expensive booster treatments. In addition, Ketamine may have quite severe side effects, even permanent neurologic injury or death in the case of the coma treatment. It has been shown that ketamine has negative stimulatory effects on cardiac function and is related to the systemic release of catecholamines (their release by sympathetic nerve endings increases the rate and force of muscular constriction of the heart), inhibition of the vagal nerve (the very thing that contributes to CRPS to begin with), and inhibition of norepinephrine re- uptake at peripheral nerves and non- neuronal tissues such as the myocardium. Heart muscle depression has been observed after high dose ketamine infusions or during repeated dosing.
It is my hypothesis that Ketamine changes the Nervous System for often long periods of time, if not permanently. No study that I could find has ever been performed to study the long term changes of Ketamine in the human body. It is my experience that for my treatment, Ketamine represents somewhat of a ‘wild card’ effect, in that it will sometimes make the patient not respond to treatment as well as other CRPS patients, especially if the Ketamine treatments have been recent.
Again, Ketamine does not address the original cause of CRPS, but rather changes the Nervous System.
Approved by the FDA in 1989, spinal cord stimulation (SCS) has become a common treatment for patients with chronic pain in their back and or limbs who have not found pain relief from other treatments. Soft, thin wires with electrical leads on their tips are placed through a needle in the back near to the spinal column. The leads are placed through a needle inserted in the back (no incision is required). A small incision is then made and a tiny, programmable generator is placed under the skin. There it emits electrical currents to the spinal column.
Some CRPS patients report a significant decrease in daily pain after getting a SCS. Others report no relief or even an increase in pain after the procedure. For some, it may work for a while, and the stop being as effective. As with any implanted device, infection can occur. The lead, extension, or neurostimulator could move within the body or push through the skin. There could be undesirable changes in stimulation. It is also possible that the implanted materials (as with any foreign object in the body) may cause an allergic or immune system response. The device might unexpectedly cease to function due to battery depletion or other causes.
Another side effect of SCS is that it may cause scarring. Scar tissue can be very detrimental to your Nervous System’s health. Nerve communication moves through cells in a wave- like pattern, rather than electricity moving through a wire. In fact, electricity in a nerve is not like an electric current at all. An electric current is a rapid flow of electrons, but electricity sweeps along the nerve as an ‘action potential’, a difference in electrical charge between the outside and the inside of the nerve43. Think of a wave moving through water, if there is a rock in that body of water. The rock will cause a ‘break’ in the wave pattern. Much like the rock, the nerve ‘wave’ cannot move through scar tissue like it moves through healthy tissue. This will often result in an increase in pain and resistance to successful treatment. In addition, it is an invasive procedure which is always risky when treating CRPS. The cost of a SCS is usually more than $50 000 with significant annual upkeep. However, insurance companies will often cover it. Spinal Cord Stimulators are not FDA approved for the treatment of CRPS.
Drug pumps, or intrathecal drug delivery devices, deliver pain medication directly to the fluid-filled area surrounding the spinal cord (called the intrathecal space). The system consists of a pump and catheter (a thin, flexible tube), both of which are surgically implanted under the skin. The pump is a round device that stores and delivers pain medication, and is typically implanted in your abdomen. The catheter is placed in a small space created by the surgeon at the spine and connected to the pump. With this system, pain medication goes directly to the pain receptors near the spine, instead of going through the circulatory system. For that reason, drug pumps offer significant pain control using just a fraction of the dose that oral medication requires.
Since this procedure requires surgery, complications (made more possible by the presence of CRPS) and/or infection may occur. Once implanted, several complications may occur with the device, such as the catheter leaking or tearing, or becoming disconnected. The pump or catheter may move or wear through the skin. These complications may require surgery. The pump may stop if the battery runs out. Drug overdose or underdose can result in serious complications and may even be life- threatening. The typical side effects of the drug being delivered should also be considered. The formation of an inflammatory mass at the tip of catheter has been reported, which may lead to serious complications, such as paralysis. The same problems with scarring that occurs with spinal cord stimulators may occur with drug pumps. In my experience, at least external scarring is rather significant in most patients. The body does not like foreign objects inside of it, and will often react to it in various adverse ways.
Sympathectomy is performed to interrupt the portion of the patient’s sympathetic nervous system (SNS) that is affected by CRPS. During sympathectomy, the sympathetic ganglia that cause CRPS pain are cut surgically, or chemically destroyed. It may also be destroyed with radiofrequency. Surgical sympathectomies are irreversible procedures. Sympathetic ganglia are collections of nerve cells that occur in clusters along the mid or lower spinal cord. It is especially recommended for patients who have received significant pain relief from sympathetic nerve blocks. Sympathetic nerve blocks involve injecting anesthetics into sympathetic nerves that are affected by CRPS. Sympathectomies are extremely controversial, as there is little evidence to fully support the efficacy of the procedure. Many doctors (including myself) deem this procedure risky due to the irreversible damage to sympathetic nerves.
This procedure causes nerve signals to be irreparably disrupted. These signals would normally travel to many different organs, glands and muscles. Sympathectomies will distort many bodily functions, including vascular responses, sweating, heart rate, thyroid function, pupil dilation, lung volume, skin temperature, and the vitally important fight or flight response. It also reduces the physiological responses to strong emotions, such as fear, alertness, arousal, and laughter. In addition, it has been shown that it may cause immune system dysfunction, as well as acquired cardiovascular disease. Chemical sympathectomies may lead to sympathetic sprouting. This may cause the pain of CRPS to return even more intensely than before. Sympathectomies are typically “last resort” procedures for patients who face edema, tissue loss, and recurrent infection.
TMS is a noninvasive method used to stimulate small, specific regions of the brain. A magnetic field generator, or “coil”, is placed near the head of the person receiving the treatment during a TMS procedure. The coil produces small electric currents in the region of the brain just under the coil. The coil is connected to a pulse generator, or stimulator, that delivers an electric current to the coil. It is hypothesized that TMS affects the Central Nervous System much the same as Ketamine does, but without all the nasty side effects. Unfortunately, while TMS does seem to provide some relief for patients, it does not seem to work for everyone and most often does not seem permanent. Some within the CRPS community have questioned whether the level and durations of relief warrant the cost involved (about $10 000 for a series, although some clinics may charge less). TMS is FDA approved for Migraines and major depression only, and not all insurance companies will cover this treatment.
The greatest risks of TMS are the rare occurrence of fainting and even less commonly, seizures, also not very common. Other unwanted effects of TMS include discomfort or pain, transient induction of a mild form of mania, transient cognitive changes (that interferes with your thinking), temporary hearing loss and impairment of working memory. It may cause problems with pacemakers.
In 2014, the FDA finally acknowledged that CRPS is indeed, a rare condition. This has vast implications for pharmaceutical companies, as this is a game changer when it comes to CRPS research. These companies may now receive attractive tax breaks, and may include fewer subjects in any studies necessary to prove the ethicacy of a drug developed specifically for CRPS. In addition, such companies may market the drug for seven years without threat of competition. This is getting a lot of corporate attention. The first company to launch such research in the USA was Grunenthal, a German- based company, and the trail medication is neridronate, also known as amino-bisphosphate. This study is expected to be completed in 2016.
Significant attention has been focused on this drug since a very small but successful trial was completed in Italy44. The inclusion for this trial was very strict, as no one whose CRPS onset was greater than four months ago was allowed to participate. This study reported a good outcome of up to a year. Surprisingly, the placebo group in this study also reported a marked initial decrease in pain. The USA study trail inclusion will not be as strict, with the exception of patients who suffer from CRPS Type 2, meaning that nerve damage can be detected. Neridronate has been used in Europe for quite some time now. Bisphosphates are a class of drugs that prevent the loss of bone mass, used to treat osteoporosis and similar diseases. Bone undergoes constant turnover and is kept in balance by specific bone cells called osteoblasts (that create bone) and osteoclasts (that destroy bone). Bisphosphonates inhibit the destruction of bone by encouraging osteoclasts to undergo cell death, thereby slowing bone loss. It does not encourage new bone growth, but simply slows down bone loss.
The side effects of this drug include muscle tremors, muscle and joint pain, inflammation of the eye, fever, cardiac arrhythmia, artrial fibrillation, thyroid problems and jaw necrosis. Since this last side effect is often glossed over, I want to make sure that we address it in detail, so that you understand the gravity of it. Necrosis means dying of the bone that form the jaw and house the teeth. This is not an uncommon side effect at all. This occurs more often when bisphosphates are administered through an IV, rather than orally. One large study found that 20% of IV bisphosphate users will develop necrosis of the jaw. There is no way to prevent this side effect. It is most often triggered by dental work after the drug has been administered, especially any kind of dental surgery. The risk remains high for the lifetime of the patient. Many dentists will not agree to work on a patient who has taken this drug, due to fear of complications. The symptoms of jaw necrosis include bad breath, lock jaw, abscesses, pockets of pus, loosening teeth, numbness in the face, feeling of heaviness in the jaw, and swelling of the gums or face.
Much hope is being focused on the current USA trial. Caution is advised, however, since the safety of taking this drug long term has not been studied, and the known side effects are potentially serious. There is no word yet on possible insurance company coverage of this treatment, nor the cost of this treatment.
Hyperbaric oxygen therapy (HBOT) is a form of treatment that is recommended for many different types of diseases and ailments. The most recognized use of HBOT is to help scuba divers recover from ‘the bends’, or decompression sickness. HBOT works as a treatment for CRPS by saturating all body tissues with oxygen. This first relieves any oxygen deprivation that has come from the swelling or tissue damage. It may also relieve swelling and increase circulation. Possible symptoms or side effects after HBOT can include fatigue, lightheadedness, lung damage, sinus damage, changes in vision (nearsightedness), lung failure, seizures, and fluid buildup in the lungs. Side effects are generally mild as long as the therapy lasts no longer than 2 hours and the pressure inside the chamber is less than 3 times that of the normal pressure in the atmosphere.
There are currently about fourteen ailments that the F.D.A. has approved HBOT as a treatment for, but CRPS is not one of them. For this reason, insurance companies will often not cover HBOT. The typical treatment series for CRPS is about 40 sessions with additional treatments after as needed. Treatment cost is typically about $250 – $300 per session. HBOT is non- invasive and typically won’t make patients worse. CRPS patients report varying degrees of success with this treatment, although many find it beneficial. One drawback is that the patient cannot always tell early on if it HBOT will work for them, which can make it a costly trial.
Few subjects (other than politics or religion) are as polarizing as the medical use of Marijuana (Cannabis) for pain, even within the CRPS community, where people understand chronic pain better than most. However, writing a book about CRPS and not discussing marijuana news will reflect poorly on me as its author. That being said, I want to make it clear that I am not firmly in either camp regarding this subject. I see both plusses and minuses on both sides. If you live in a state where the use of marijuana is illegal, I am obviously not advising you to start using it.
As we all know, the use of medical marijuana has been approved by only a few states in the USA, although the movement to legalize it is gaining more steam, and the issue is slowly making it onto more ballots countrywide. Worldwide, it is illegal in most countries although some countries have decriminalized it, which basically means that these counties consider it a ‘soft’ drug and have turned a blind eye to its usage (the Netherlands, for instance).
At least one study has shown a positive effect on sleep as well as pain with moderate daily Cannabis usage.46 However, even this study cautioned that the long- term effects of marijuana, as well as any addictive components, have not been studied yet. Although the smoke from burning marijuana flowers contains several cancer- causing compounds, similar to those found in tobacco smoke, smoking marijuana has been shown to be vastly less damaging to the lungs than tobacco by at least one very large scale study48. It is thought that the reason for this is that the smoke from marijuana contains several unique compounds called cannabinoids (e.g. THC and CBD) which have been shown to have significant anti- cancer and anti- tumor effects. Nevertheless, smoking marijuana may still be irritating to the lungs, causing conditions like bronchitis and asthma. For this reason, vaporizers are recommended for most people using it for medicinal purposes. Vaporizers greatly reduce the risk of airway irritation.
No matter how marijuana enters your body, it affects almost every organ in your body, as well as your nervous system and immune system. Smoking pot can increase your heart rate by as much as two times for up to three hours. Other effects include feeling ‘high’, red eyes and dilated pupils, increased appetite, slowed reaction time (making it dangerous to drive), dry mouth, dizziness, shallow breathing, feelings of paranoia, anxiety, depression, short term memory loss, and an ongoing cough.
Marijuana can be addictive for some people. Even if you buy marijuana from a legal, state regulated dispensary, it is impossible to know with 100% certainty how much THC it contains, making its effects and potential for addiction hard to predict. If you are male, marijuana can lower your libido, sperm count and quality. It has been shown by some research that there is a link between marijuana use and some mental health problems, such as depression and suicidal thoughts, although this research remains controversial. Unfortunately, very few truly objective parties choose to study the effects of long term marijuana use, which greatly impacts the study outcomes, in my opinion. The long- term effects of possible toxicity in the brain has not been studies adequately.
The human body is designed to function a certain way without outside interference. Besides good nutrition and water, as well as sunshine and oxygen, it really requires little to self- regulate. We were not designed to inhale a substance every day, ingesting chemicals that alter the way our minds work and our bodies function every day. However, it is hard to come by a better reason to do so than suffering from the pain of CRPS every day. In addition, it is much less harmful than the drugs CRPS patients take to control pain every day. In my opinion, you should be honest and mindful about your daily usage. Some people fall in the habit of getting high first thing in the morning, every day. Gauge your usage while using your pain as a guide. Use it as needed, and not just because it becomes a way of life. Treat it with the same respect that you treat any other chemical that enters your body.
New CRPS Treatments
Our Groundbreaking Non-Invasive Approach to CRPS
I set out on a journey ten years ago that made treating the nervous systems of those suffering from CRPS (Complex Regional Pain Syndrome) not only a part of my life as a chiropractic physician, but my passion and my mission.
My first CRPS patient was a man named Carlos, who suffered from full body CRPS. This case revealed to me how complicated but also rewarding treating patients who suffer from CRPS can be. I have kept in touch with Carlos through the years, and I’m delighted to say that as of today, Carlos is still in remission. In the past ten years, as my patients have shared their results, patients have come to me from all over the USA and the world.
The first question patients usually is “is your system like ____“ (fill in the blank). Is your healing system like Calmare? Is your system like Ketamine? Is it like Mirror Therapy? The simple answer to this question is that my system I have designed is not like any other system. Since I treated Carlos, I have developed a simple formula I use in the ongoing development of my treatment. I can sum it up in the following way:
My sole purpose in treating the human body is to remove anything that may interfere in the nervous system’s ability to heal the body from within.
Any treatment that has shown marked (and I do mean marked) success in this department is worth a second look. To this end, I have always maintained that one of the most powerful tools any doctor can arm themselves with is an open mind. When we are closed to new ideas, we are closed to growth. Through the years, I have adopted systems and discarded systems. This has never once meant that anything I used didn’t work, it just meant that it didn’t work consistently. Of course, there is no medical treatment that I am aware of that is universally successful. After all, I am treating the marvelous human body, not a predictable machine. However, if I find a promising treatment, I examine it, test it against our old treatments and if it works better than my old way, I replace it. In this way, the model I used ten years ago is very different from the one I use now.
That brings me to the next question. What exactly do we do? I will attempt to explain as briefly as possible.
My Unique Approach to CRPS
The treatment approach I have designed is deeply rooted in my basic philosophy as a chiropractor. Chiropractors are known by the public to “pop” backs and necks, because they hurt. However, what the public generally does not understand is that our healing art stems from the belief that the body is a self-healing organism, capable of surviving and healing even catastrophic injuries.
Most accepted treatments for CRPS are rooted in pain control. While the need for these is obvious, they also do not offer long-term solutions. When the drug or chemical compound’s effect runs out, the pain returns. Spinal Cord Stimulators are a notable exception to this rule. However, in my experience, Spinal Cord Stimulators, even when successful, merely take the edge off the pain. Neridronic acid is a new treatment currently making its way to the US. We know for certain that it may have severe side effects and does change the structure of the bones permanently. In addition, it does not work for everyone, although it has proven to work miraculously well for some. No long-term studies have been done on this treatment. Of course, the same may be said for our system. The difference, however, is that I require that none of my treatments alter the normal function of the human body, but only enhance its function.
Vagus Nerve Stimulation
One of the cornerstones of our system is vagus nerve stimulation. In our clinic, we use a technique I have personally developed to decrease pressure on the Vagus nerve. The Vagus nerve is one of the twelve cranial nerves that generally control senses like smell, balance, taste and sight. The Vagus nerve is the 10th cranial nerve and it is vastly important. It controls inflammation of the body (including nerves), GI function and immune function, to name a few. The autonomic nervous system (the automatic nervous system) is divided into two parts: Sympathetic (fight or flight) and Parasympathetic (rest and digest). The Vagus nerve contains parasympathetic fibers. In my experience, virtually 100% of CRPS patients suffer from malfunction of the Vagus nerve to at least some degree, with sympathetic dominance of their autonomic nervous system, rather than a balance between Sympathetic/Parasympathetic.
This, of course, explains why so many patients CRPS patients suffer from symptoms associated with cranial nerve dysfunction, such as sensitivity to light and sound. Also, it explains the very common failure of the digestive tract in CRPS patients, generally a symptom that is regarded as a separate diagnosis in the medical community, requiring a separate treatment.
The other parts of my system are like a tool bag full of different tools. Most patients will require a customized approach, based on their unique circumstances. Please note that in my experience, our system is like a cookie recipe. You cannot pick and choose individual ingredients and expect the same outcome as when all the treatments are used together. Synergy is vastly important, where one part is exponentially more powerful when part of my system.
Following is a brief mention of a few of the tools we use:
Detoxification (based on patient tolerance)
A functional blood analysis. Our doctor who specializes in this specifically looks for signs of a viral and/or bacterial infection. For example, patients who suffer from CRPS often will also suffer from a chronic Epstein Barr Viral (EBV) infection, making long-term healing unlikely unless the infection is addressed. Chronic bacterial bladder infections will also impede healing, and are often overlooked. Blood is not drawn unless the patient is considered stabilized, as a needle prick may spread CRPS in unstable cases.
Magnetic Resonance Therapy is used to calm the nervous system and decrease pain, in order to “set the table” and prepare the body to accept other therapies.
Emotional healing therapies. I have a doctor on our team who specializes in neutralizing the effect of emotional stress on the Central Nervous System. In our experience, most CRPS patients suffer from severe PTSD and fear, as they no longer trust their bodies to naturally be healthy. This course provides our patients with powerful tools to influence their lives and their health.
Neuromuscular Re-education, FDA approved for relaxation of muscle spasms, prevention of muscle atrophy, muscle re-education and increasing range of motion. The patient is connected to a machine that uses Direct Current (patented in a way to not cause the nervous system to “guard”) while put through specific rehabilitative exercises. This process is overseen by an experienced and dedicated therapist, familiar with your case. You will grow very close to your therapist and the day you graduate, they will be right by your side to watch you ring the bell (more about that later).
Sound wave technology is used to break up adhesions and scar tissue, both of which may impede healing to the body as a whole.
Click here to view more of the Treatment Modalities used at Spero Clinic.
We like to refer to ourselves as the Anti-Clinic
I like to refer to our clinic as the “anti-clinic”. What does this mean? Most clinics are quiet environments where patients do not interact much with each other. In our clinic, I encourage and promote bonding among our patients. I have found that when patients can encourage each other in a “buddy like” system, it is a central part to a patient’s recovery. I have a tradition where new patients meet outgoing patients to discuss the treatments, what to expect, and provide encouragement made possible because of their own progress. We encourage hugs, laughter, and humor all around.
My staff was handpicked from all walks of life. Some were waiters, some were patients, and some worked with world-class athletes. In my experience, the most important quality a staff member can possess is empathy and compassion for those who suffer. Virtually everything else can be taught. While we all wear scrubs, it is not unusual to spot piercings, tattoos, and pink hair among our staff. We definitely focus on the things that matter most and don’t waste our time on the little things that don’t.
Does our system work for everybody?
As with every treatment, my system is not universally successful. It is my strong position that we do not treat specific conditions, but bring healing to the central nervous system. In addition to CRPS, many of my patients suffer from other conditions like Ehlers Danlos Syndrome (EDS) and Postural Orthostatic Tachycardia Syndrome (POTS). The body knows how to heal from the inside out, sometimes it just needs a tour guide. If you look at my clinic’s Facebook page, you will see many videos of people “ringing the bell”. This is a tradition where my patients and staff gather when a patient graduates to their satisfaction. In most cases, that means that my patients are leaving my clinic pain-free. Of course, not everybody rings the bell. However, if you look at the many success stories you will understand that my approach should be more widely accepted as a whole, as an alternative to the philosophy that the body should be healed from the outside.
Why is my system not more widely accepted?
My system is a complicated one, fueled by years of experience and trial and error. I am fully aware that it is an effective one that should be widely available across the world. While this is my ultimate goal, it will take years to get there. As we take the first steps in this direction, for now, patients have to travel to us from distant states and countries.
Another common question is: “I have had CRPS for longer than a year. Is there still hope for me?” Yes! In my experience, time passed has no effect on the effectiveness of my treatment.
Please know that every single patient that recovers should bring you enormous hope. Their bodies are not more special, more magnificent than yours. In my clinic, I refer to “white crow moments”: you only have to see one white crow to know that not all crows are black. No matter what, you have to keep your hope alive! This must happen if you are to recover.
What does CRPS remission look like?
Our main focus is to help patients enter remission by restoring the balance to the Nervous System.
Some people experience complete remission and some people find that it is now possible to lead a fairly normal life with manageable pain levels. The definition of success is different for every person.
We believe true remission means living without limitations. It means embracing life and being able to do all the activities you used to do, and maybe even more.
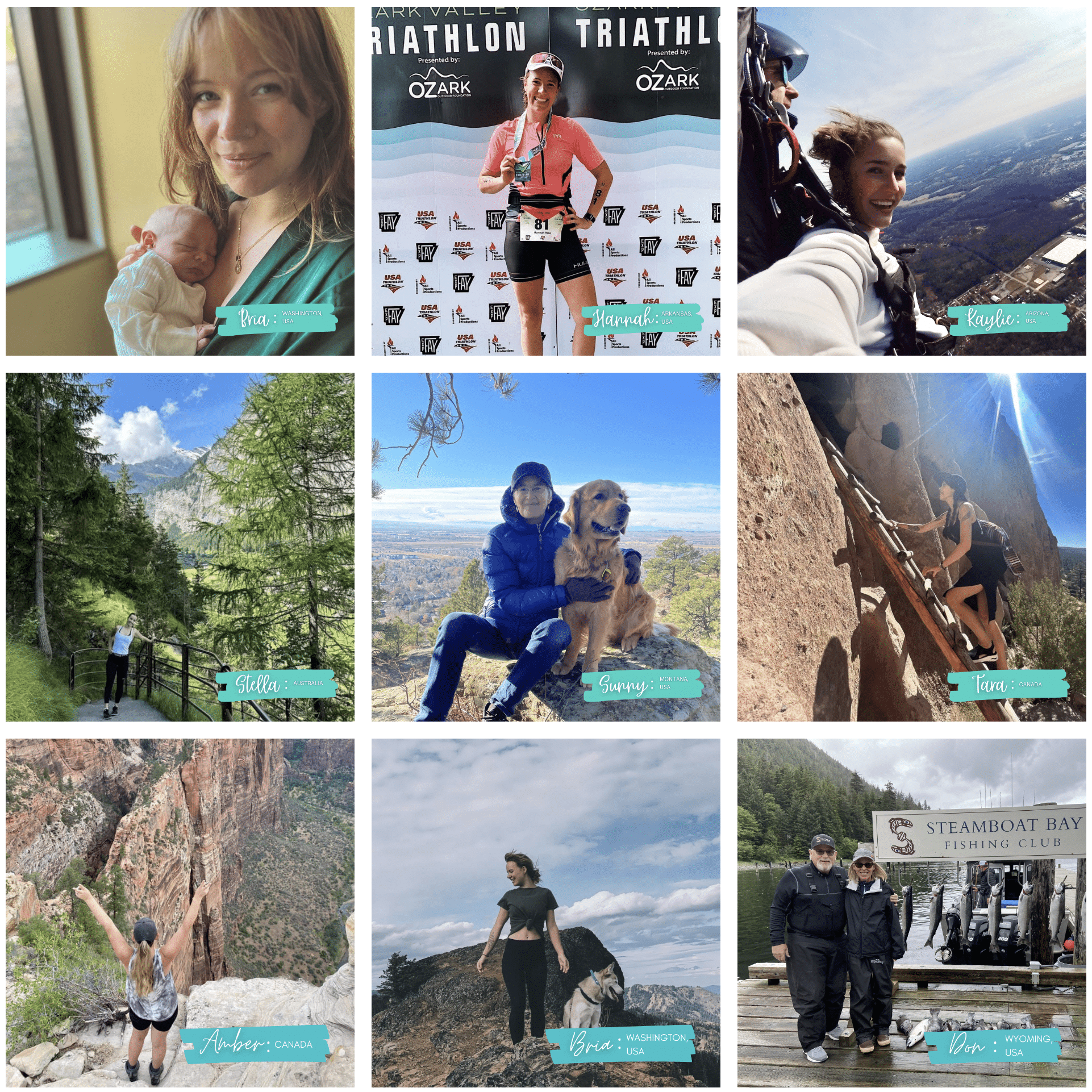
Check out our What does remission look like? page to browse pictures provided by former patients of ours, showing some of the activities that they can now enjoy without pain or fear. We hope these images inspire you and give you hope!
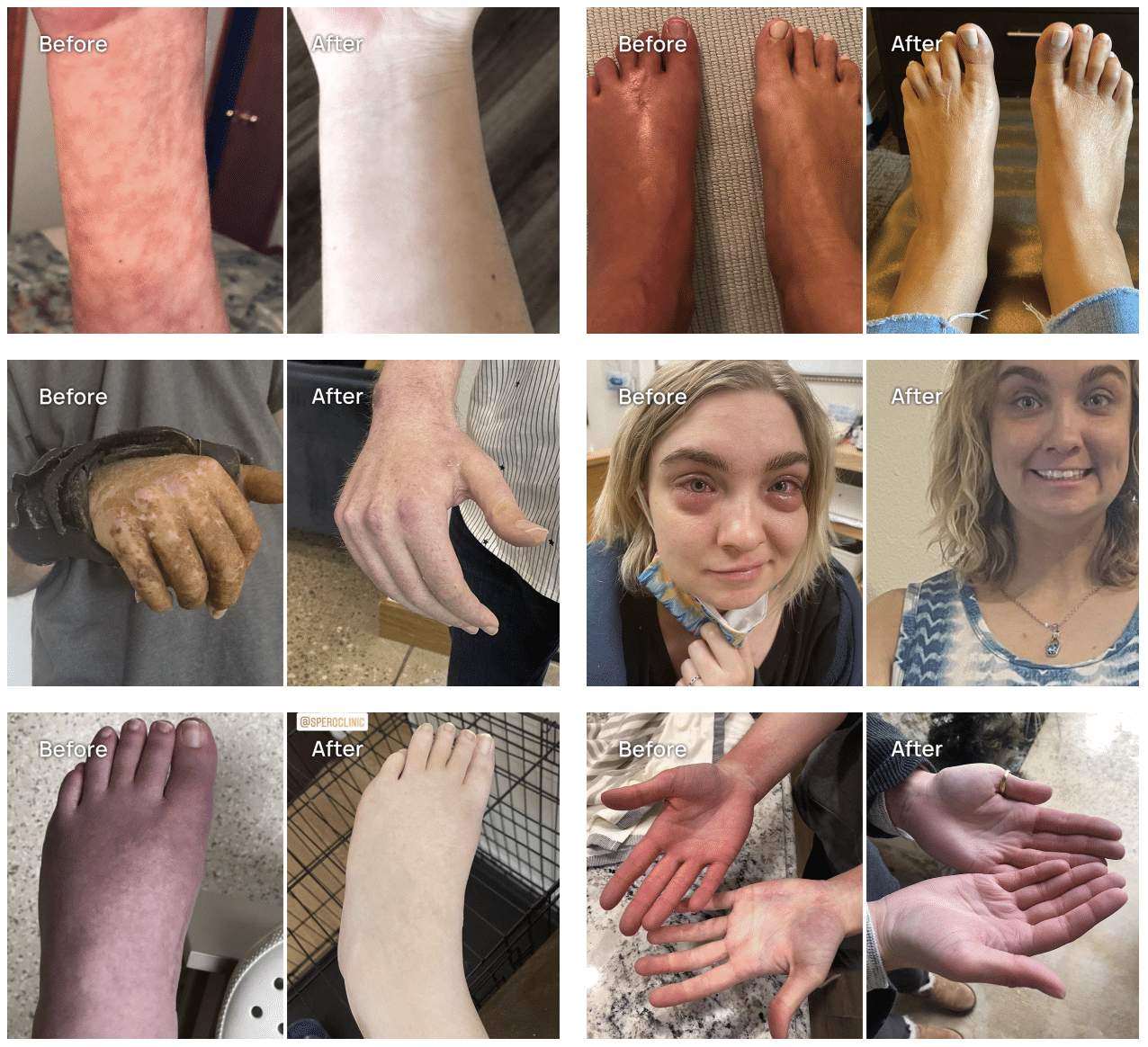
See how others like you have found relief at the Spero Clinic. Read Spero Clinic patient success stories and their experiences from start to finish, here.
Hope for CRPS
Dr. Katinka and the staff at the Spero Clinic have helped 1000+ CRPS patients to enter remission and start living normal lives again.
Our treatment methods have proven to be effective and our diagnostic system enables us to know right away whether the treatment will be effective. Schedule a free consultation with our CRPS specialists today. Call now.
 I set out on a journey ten years ago that made treating the nervous systems of those suffering from CRPS (Complex Regional Pain Syndrome) not only a part of my life as a chiropractic physician, but my passion and my mission.
I set out on a journey ten years ago that made treating the nervous systems of those suffering from CRPS (Complex Regional Pain Syndrome) not only a part of my life as a chiropractic physician, but my passion and my mission. 
 One of the cornerstones of our system is vagus nerve stimulation. In our clinic, we use a technique I have personally developed to decrease pressure on the Vagus nerve. The Vagus nerve is one of the twelve cranial nerves that generally control senses like smell, balance, taste and sight. The Vagus nerve is the 10th cranial nerve and it is vastly important. It controls inflammation of the body (including nerves), GI function and immune function, to name a few. The autonomic nervous system (the automatic nervous system) is divided into two parts: Sympathetic (fight or flight) and Parasympathetic (rest and digest). The Vagus nerve contains parasympathetic fibers. In my experience, virtually 100% of CRPS patients suffer from malfunction of the Vagus nerve to at least some degree, with sympathetic dominance of their autonomic nervous system, rather than a balance between Sympathetic/Parasympathetic.
One of the cornerstones of our system is vagus nerve stimulation. In our clinic, we use a technique I have personally developed to decrease pressure on the Vagus nerve. The Vagus nerve is one of the twelve cranial nerves that generally control senses like smell, balance, taste and sight. The Vagus nerve is the 10th cranial nerve and it is vastly important. It controls inflammation of the body (including nerves), GI function and immune function, to name a few. The autonomic nervous system (the automatic nervous system) is divided into two parts: Sympathetic (fight or flight) and Parasympathetic (rest and digest). The Vagus nerve contains parasympathetic fibers. In my experience, virtually 100% of CRPS patients suffer from malfunction of the Vagus nerve to at least some degree, with sympathetic dominance of their autonomic nervous system, rather than a balance between Sympathetic/Parasympathetic.
 As with every treatment, my system is not universally successful. It is my strong position that we do not treat specific conditions, but bring healing to the central nervous system. In addition to CRPS, many of my patients suffer from other conditions like Ehlers Danlos Syndrome (EDS) and Postural Orthostatic Tachycardia Syndrome (POTS). The body knows how to heal from the inside out, sometimes it just needs a tour guide. If you look at my clinic’s Facebook page, you will see many videos of people “ringing the bell”. This is a tradition where my patients and staff gather when a patient graduates to their satisfaction. In most cases, that means that my patients are leaving my clinic pain-free. Of course, not everybody rings the bell. However, if you look at the many success stories you will understand that my approach should be more widely accepted as a whole, as an alternative to the philosophy that the body should be healed from the outside.
As with every treatment, my system is not universally successful. It is my strong position that we do not treat specific conditions, but bring healing to the central nervous system. In addition to CRPS, many of my patients suffer from other conditions like Ehlers Danlos Syndrome (EDS) and Postural Orthostatic Tachycardia Syndrome (POTS). The body knows how to heal from the inside out, sometimes it just needs a tour guide. If you look at my clinic’s Facebook page, you will see many videos of people “ringing the bell”. This is a tradition where my patients and staff gather when a patient graduates to their satisfaction. In most cases, that means that my patients are leaving my clinic pain-free. Of course, not everybody rings the bell. However, if you look at the many success stories you will understand that my approach should be more widely accepted as a whole, as an alternative to the philosophy that the body should be healed from the outside.